 News
News Diagnosis and treatment of pouchitis
Overview
This article describes the process for the diagnosis and treatment of pouchitis as recommended by St. Mark’s hospital, London – the UK National bowel hospital.
Symptoms
A small percentage of people with a j pouch will at some stage experience pouchitis. [The incidence of pouchitis is 20% at one year and up to 40% at 5 years. 10 to 15% of patients with pouchitis experience chronic pouchitis, which is classified as either ’treatment responsive’ or ’treatment refractory’. 1]
Symptoms of pouchitis are not dissimilar to those experienced by patients whose original diagnosis was ulcerative colitis (UC). For example, abdominal pain, cramping, increased frequency, urgency and bleeding.
Diagnosis
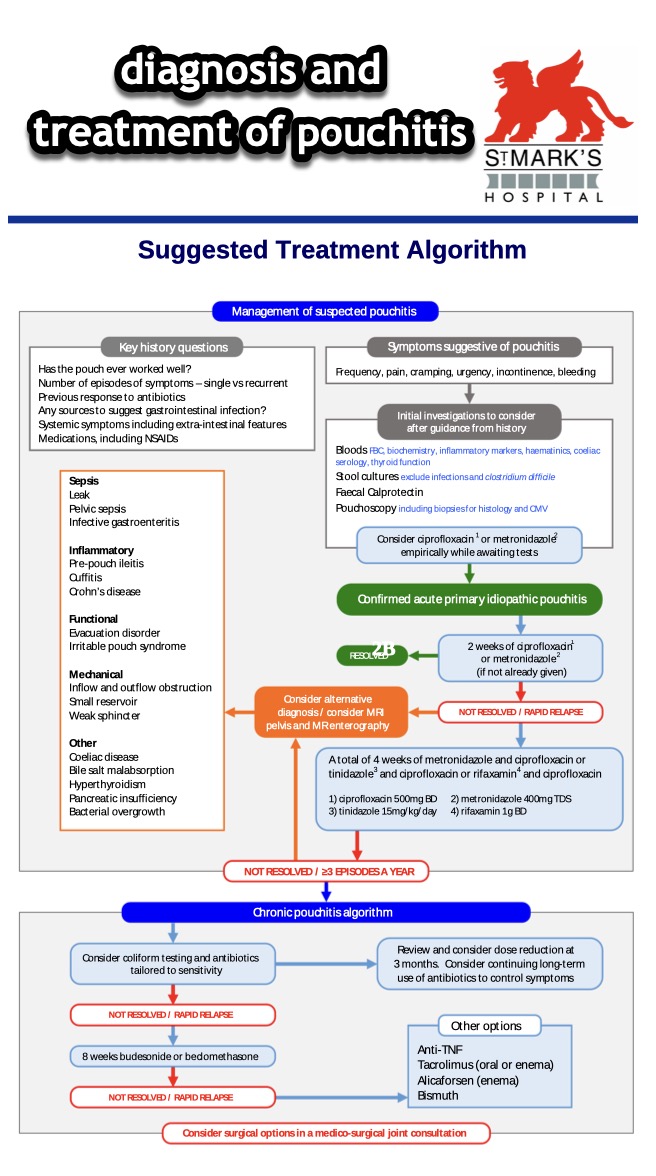
Initial diagnosis is based on advanced history taking and assessment of symptoms. This is why it is important that patients speak to someone experienced in pouches, as otherwise they risk being misdiagnosed. Blood tests and pouchoscopy may be considered subject to the history taking and assessment findings.
Treatment
In most cases pouchitis responds well to antibiotics. [two weeks Ciprofloxacin and metronidazole are the most commonly used, often generating a rapid dramatic response. 1] This may be followed up with further four weeks of antibiotics if not resolved or rapid relapse.
In the event that symptoms are not responsive to the antibiotics, investigations into alternative possible diagnosis would be carried out.
For the complete treatment algorithm, including the treatment of chronic pouchitis, refer to the St. Mark’s hospital Suggested Treatment Algorithm below.
You can download a copy of the treatment algorithm below :-

References:
1 From the paper “Systematic review: management of chronic refractory pouchitis with evidenced based treatment algorithm” published on Research gate.
You can read the actual paper on Research gate by clicking here or the image below.











You must be logged in to post a comment.